

Enough is Enough, Or Is It?
Paradigms in Micronutrient Sufficiency: A Comparative Analysis of Vitamin Deficiency Norms and Clinical Biomarkers Across the United States, Russia, Japan, and Italy

The assessment of national health is an endeavor that transcends basic demographic metrics such as infant mortality and life expectancy, extending deep into the granular, biochemical realities of the populations in question. Global health indices frequently evaluate and rank nations based on an aggregate of environmental quality, healthcare access, morbidity burdens, and lifestyle factors. However, an under-explored aspect of these overarching rankings is the biochemical baseline accepted as “normal” by a nation’s medical and scientific establishment.
Clinical reference intervals for essential micronutrients like Vitamin D, Vitamin B12, and Folate vary significantly across geopolitical borders. These variations are not merely statistical artifacts or the result of differing laboratory assay calibrations; they reflect divergent public health philosophies, historical dietary patterns, and contrasting policies regarding mass food fortification.
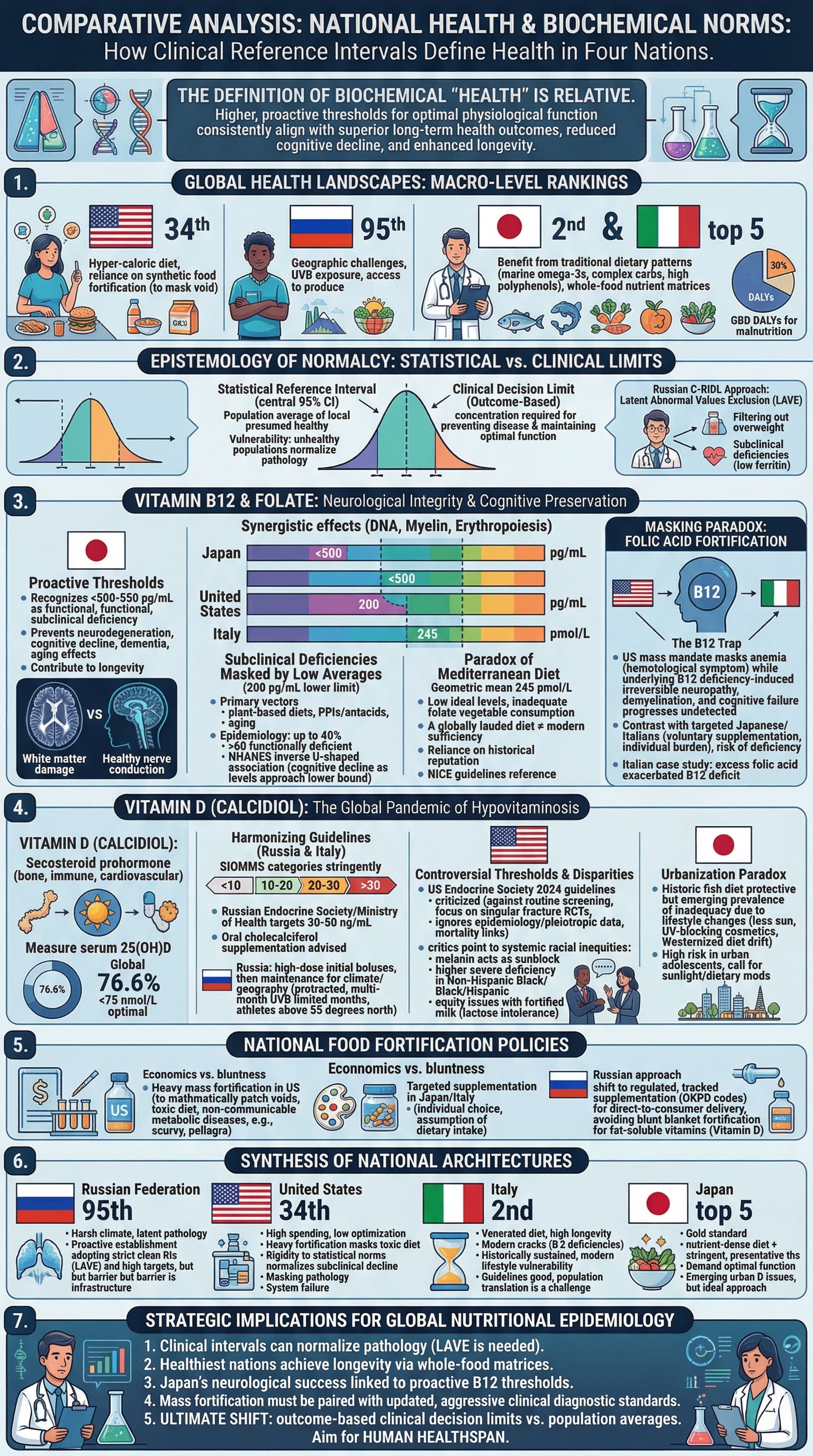
This research report attempts to provide a comparative analysis of vitamin deficiency norms, clinical blood test markers, and nutritional epidemiology across four distinct landscapes: the United States, the Russian Federation, Japan, and Italy. By examining these nations which span the spectrum from the lowest-ranked developed nations in global health to the highest, the analysis reveals a profound second-order insight. The definition of biochemical “health” is relative, and nations that enforce higher, more proactive threshold markers for optimal physiological function consistently align with superior long-term health outcomes, reduced cognitive decline, and enhanced longevity.
1. The Macro-Landscape of Global Health and Nutritional Epidemiology
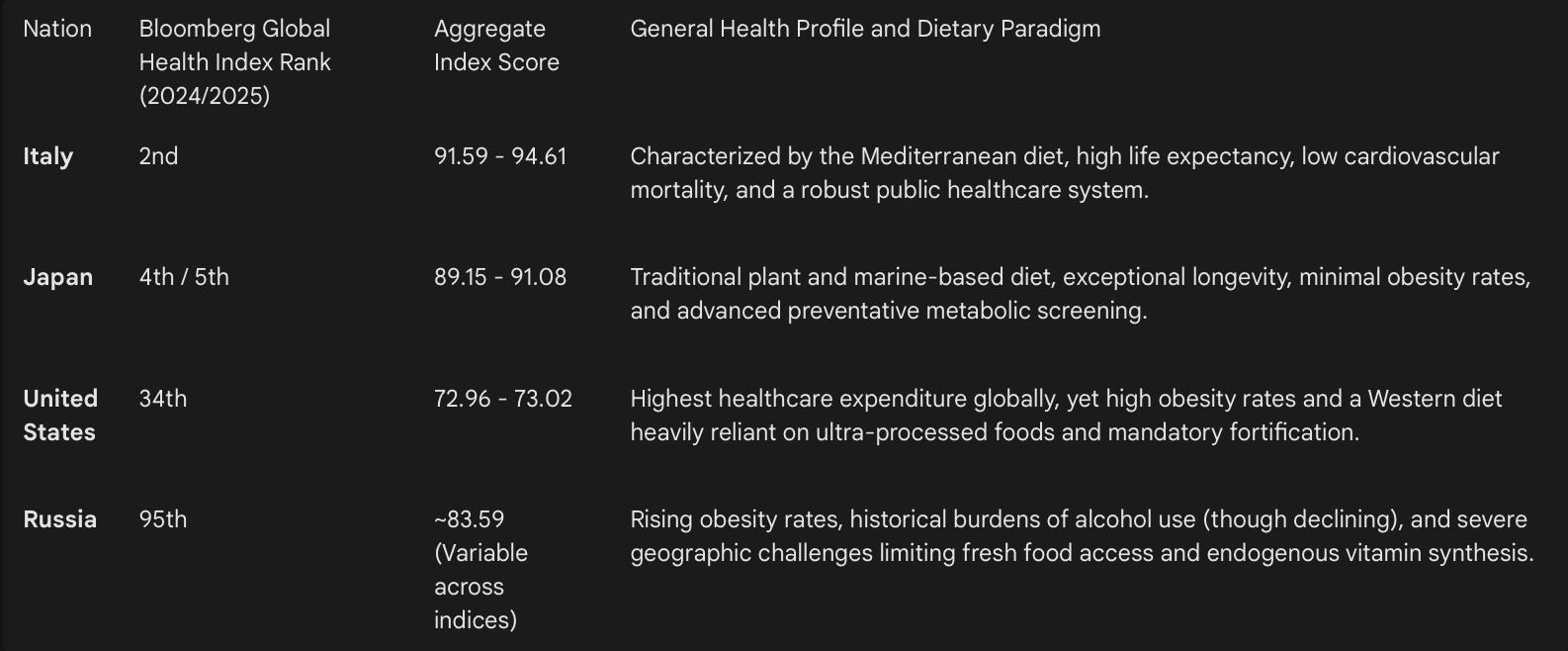
To appropriately contextualize the biochemical data, it is necessary to first establish the overarching health rankings of the nations under review. The Bloomberg Global Health Index, the CEOWorld Global Health Index, and the Legatum Prosperity Index evaluate countries based on a complex matrix of life expectancy, environmental conditions, and health risks such as obesity, tobacco use, and sedentary lifestyles. Furthermore, the Global Burden of Disease (GBD) framework assesses the disability-adjusted life years (DALYs) associated with nutritional deficiencies, providing a baseline for the global burden of malnutrition in all its forms.
The data indicates a stark divergence between the top-tier nations (Italy and Japan) and the lower-tier nations (the United States and Russia). While Italy and Japan benefit from traditional dietary patterns rich in marine omega-3 fatty acids, complex carbohydrates, and high-polyphenol profiles, the United States consumes a hyper-caloric diet that necessitates artificial food fortification to prevent widespread acute clinical deficiencies. The Russian Federation faces unique geographic and infrastructural challenges that limit year-round access to fresh produce and adequate ultraviolet-B (UVB) exposure, exacerbating risks for specific micronutrient deficits across its vast population.
A deeper epidemiological insight emerges when correlating these macroscopic rankings with microscopic clinical data. Nations with the highest health indices often rely on whole-food nutrient matrices and maintain stringent markers for biochemical sufficiency. Conversely, nations with lower indices rely heavily on synthetic fortification to mask the nutritional void of ultra-processed diets. Consequently, the clinical reference ranges in these lower-ranked countries often adapt to the population’s compromised median. This leads to a dangerous epidemiological phenomenon where a statistically “normal” blood test in a metabolically unhealthy country may represent a state of subclinical, pathological deficiency in a healthier country.
The Global Burden of Disease (GBD) 2021 data confirms that while the overall global burden of severe nutritional deficiencies has declined significantly since 1990 (evidenced by a 51.9% reduction in the age-standardized DALY rate), the prevalence of subclinical deficiencies in high-income and middle-income nations remains a persistent threat to global public health.
2. The Epistemology of Normalcy: Statistical Reference Intervals Versus Clinical Decision Limits
The foundation of modern diagnostic medicine rests upon the clinical laboratory reference interval (RI). Traditionally, RIs are calculated based on the central 95% confidence interval (the 2.5th to 97.5th percentiles) of a presumed healthy local population. The International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) and the Clinical and Laboratory Standards Institute (CLSI) dictate that laboratories should ideally establish these ranges locally, using rigorous methodological protocols to account for demographic and genetic variations.
However, this statistical methodology harbors a critical biological vulnerability. If the reference population suffers from endemic, low-grade malnutrition, widespread chronic inflammation, or latent micronutrient depletion, the resulting reference range mathematically normalizes pathology.
2.1 Latent Pathology and the Russian C-RIDL Methodological Adjustments
Recent scientific efforts within the Russian Federation elegantly illustrate the complexities of establishing accurate, biologically meaningful RIs. Russian researchers, strictly following the harmonized protocol of the IFCC Committee on Reference Intervals and Decision Limits (C-RIDL), recruited healthy adults to establish RIs for complete blood counts, iron markers, Vitamin B12, and folate.
During the cohort selection process, a significant challenge emerged: the high baseline prevalence of latent iron deficiency anemia and obesity within the Russian population. The researchers discovered that utilizing standard statistical derivations without aggressive exclusion criteria resulted in severely skewed, artificially lowered ranges. To counteract this, the researchers applied the latent abnormal values exclusion (LAVE) method. This secondary exclusion mechanism filtered out individuals with subclinical deficiencies (such as low ferritin levels without overt anemia) and those with a Body Mass Index (BMI) greater than 28 kg/m², prior to calculating the baseline.
Even with these rigorous exclusions, the derived Russian RIs for certain parameters, such as total leukocyte and neutrophil counts, mirrored the lower ranges typically found in developing African nations, highlighting the inescapable impact of underlying population health on statistical norms. The Russian methodology underscores a third-order insight: statistical normalcy is not synonymous with biological optimality. Without applying aggressive secondary exclusion methods like LAVE, national healthcare systems risk embedding systemic malnutrition into their diagnostic algorithms.
2.2 The Shift Toward Optimal Clinical Decision Limits
In contrast to statistical reference intervals derived from population averages, there is a growing, necessary movement in clinical biochemistry to utilize “clinical decision limits.” These limits are not based on the mathematical average of a local population but are instead anchored to the specific biomarker concentration required to prevent downstream disease states and maintain optimal physiological function.
This fundamental divergence in methodology i.e statistical population averages versus optimal functional outcomes is the primary driver of the massive discrepancies in Vitamin B12 and Vitamin D diagnostic thresholds observed between the United States, Japan, Italy, and Russia.
3. Vitamin B12 and Folate: Neurological Integrity, Cognitive Preservation, and the Threshold Divergence
Vitamin B12 (cobalamin) and folate (Vitamin B9) are highly synergistic water-soluble vitamins critical for DNA synthesis, erythropoiesis, amino acid metabolism, and the maintenance of the myelin sheath surrounding central and peripheral neurons. Deficiencies in either nutrient impair the methionine synthase pathway, leading to the accumulation of homocysteine and methylmalonic acid (MMA). Overt, end-stage deficiencies lead to megaloblastic (macrocytic) anemia and irreversible neurological damage, including cognitive decline, memory loss, dementia, and combined degeneration of the spinal cord.
3.1 The Japanese Paradigm: Proactive Thresholds for Cognitive Preservation
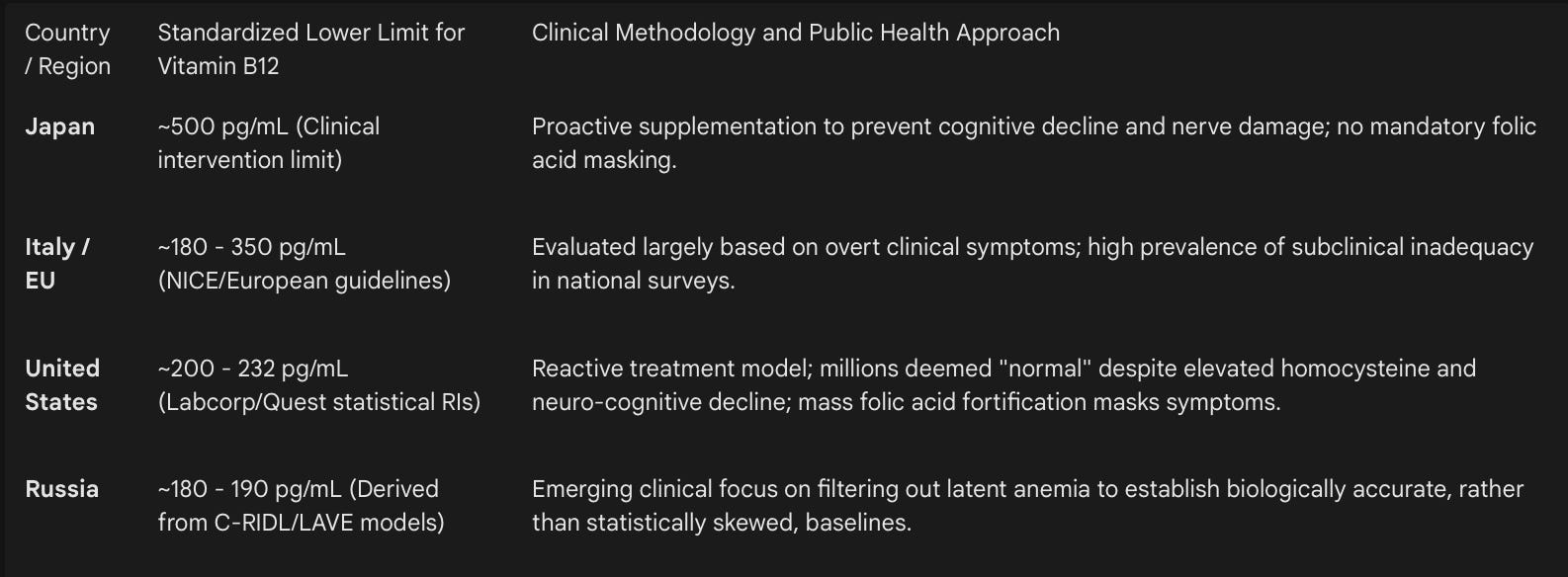
Japan presents the most aggressive, preventative public health stance on Vitamin B12 clinical thresholds globally. While the World Health Organization (WHO) and standard American laboratory chains often define the lower limit of normal serum B12 as approximately 200 pg/mL, clinical practices in Japan recognize levels below 500 to 550 pg/mL (roughly equivalent to 369 to 405 pmol/L) as indicative of functional, subclinical deficiency requiring intervention.
This elevated threshold is not arbitrary; it is rooted in advanced neurocognitive research. Extensive clinical studies link serum B12 levels between 200 pg/mL and 500 pg/mL which is a broad range considered perfectly healthy and normal in the United States with insidious neurological degradation. For instance, researchers at the University of California, San Francisco (UCSF) evaluated older, healthy volunteers with B12 levels situated in this “normal” American range. The study found that these individuals exhibited significantly slower nerve conduction in visual pathways, reduced cognitive processing speeds, and visibly increased white matter damage on brain MRI scans.
The Japanese medical community recognizes that waiting for overt hematological symptoms (such as anemia) to manifest is a failure of preventative medicine. In Japan, the willingness to aggressively supplement patients who exhibit “normal” levels by US standards, but low-optimal levels by Japanese standards, is widely hypothesized by neuroscientists to be a contributing factor to the nation’s exceptional longevity and lower age-adjusted rates of Alzheimer’s disease and cognitive dementia. By setting the clinical decision limit at 500 pg/mL, Japanese medical standards prioritize the prevention of downstream metabolic cascades and demyelination long before irreversible structural brain changes occur.
3.2 The United States: Subclinical Deficiencies Masked by Averages
In the United States, major national laboratory chains such as Quest Diagnostics and Labcorp define normal B12 levels broadly, spanning from 200 to 1,000 pg/mL or 232 to 1,245 pg/mL, respectively. Consequently, an older American patient presenting to a primary care physician with symptoms of mental fogginess, memory issues, or peripheral neuropathy with a B12 level of 250 pg/mL will typically be informed that their levels are strictly “normal,” precluding any further diagnostic evaluation or supplementation.
Epidemiological estimates suggest that a staggering 40% of Americans over the age of 60 are operating with functionally deficient B12 levels, despite falling within the accepted statistical reference range. This widespread, unacknowledged depletion is driven by several primary vectors in the US population:
Dietary Shifts: The increasing mainstream adoption of plant-based and vegan diets, which lack natural sources of bioavailable cobalamin.
Pharmaceutical Interference: The pervasive, chronic use of proton pump inhibitors (PPIs) and antacids (e.g., omeprazole, pantoprazole), which suppress the gastric acid and intrinsic factor required to cleave B12 from dietary animal proteins.
Aging and Gastrointestinal Health: Increasing rates of atrophic gastritis and gut dysbiosis reduce the mucosal production of intrinsic factor, essential for terminal ileum B12 absorption.
A comprehensive cross-sectional analysis of older US adults (aged 60 and above) from the National Health and Nutrition Examination Survey (NHANES) cohort confirmed these risks. Utilizing artificial intelligence unsupervised learning and restricted cubic spline models, researchers identified a statistically significant inverse U-shaped association between B12/folate status and cognitive function. Outcomes on the Consortium to Establish a Registry for Alzheimer’s Disease Word Learning (CERAD-WL) and Delayed Recall (CERAD-DR) tests declined precipitously as B12 concentrations approached the lower statistical bounds. The rigid adherence to outdated, population-derived statistical norms in the United States represents a systemic failure to treat neurological decline preventatively.
3.3 Italy and the Paradox of the Mediterranean Diet
Italy consistently ranks as one of the healthiest nations globally, an achievement primarily attributed to the widespread historical adherence to the Mediterranean diet. However, recent and highly granular nationwide biochemical surveys expose severe gaps in B-vitamin status, challenging the assumption that geographic dietary patterns guarantee modern micronutrient sufficiency.
The Fourth Italian National Food Consumption Survey (IV SCAI 2017–2020) and data from the ongoing CUORE Project indicate that the contemporary Italian diet, while still heavily cereal-based, suffers from notable nutritional imbalances, including inadequate dietary fiber and massive deficiencies in essential vitamins.
A specific regional study conducted in middle-southern Italy assessing adult blood donors found alarming biochemical realities. The geometric mean for serum B12 was a mere 245.0 pmol/L (approximately 332 pg/mL). Only 16.3% of the cohort demonstrated ideal levels of Vitamin B12, and an inadequate baseline consumption of folate-rich vegetables was rampant across both genders. Furthermore, utilizing the UK’s National Institute for Health and Care Excellence (NICE) guidelines which are frequently utilized as a benchmark in European contexts, the recommended absolute deficiency threshold is set at 180 ng/L (pg/mL), with a “possible deficiency” range extending up to 350 ng/L. By this metric, a substantial majority of the Italian population operates in a constant state of possible deficiency.
This reveals a profound, counter-intuitive insight: a globally lauded dietary pattern (the Mediterranean diet) does not inherently guarantee micronutrient sufficiency in the modern era if the population slowly drifts toward refined, nutrient-depleted cereals and moves away from highly diverse, micronutrient-dense biological inputs. The low B-vitamin status in Italy highlights a critical vulnerability in public health planning: That strict reliance on historical dietary reputations rather than aggressive modern bio-monitoring leads to invisible epidemics of insufficiency.
3.4 The Masking Paradox: Folic Acid Fortification and Undetected Neuropathy
The discrepancies in clinical biomarkers across these nations are deeply influenced by national food fortification policies. The World Health Organization (WHO) provides global, evidence-informed guidelines for the mass fortification of staple foods, specifically recommending the addition of iron, zinc, folic acid, and Vitamin B12 to wheat and maize flour to combat endemic malnutrition.
The United States has long championed mandatory mass fortification. Following the discovery of the definitive link between maternal folate deficiency and fetal neural tube defects (NTDs), the US mandated the fortification of all enriched grain products with synthetic folic acid in 1998. This public health intervention was undeniably successful in eradicating widespread, severe folate deficiency and dramatically reducing NTD incidence. However, this strategy introduces severe secondary biochemical complications due to the interdependent nature of the B-vitamin complex.
High intakes of synthetic folic acid can effectively cure the megaloblastic (macrocytic) anemia caused by Vitamin B12 deficiency. When the primary hematological symptom (anemia) is masked by fortified folic acid, the underlying B12 deficiency goes entirely undetected by standard complete blood counts (CBCs). Meanwhile, the B12-dependent neurological damage continues unabated, progressing until irreversible neuropathy, demyelination, and cognitive failure occur.
Since the United States relies on aggressive mass folic acid fortification while simultaneously maintaining notoriously low diagnostic thresholds for B12 normalcy (200 pg/mL), the American population is highly susceptible to this specific, devastating biochemical trap. Millions of individuals with sub-optimal B12 may show perfectly normal red blood cell indices due to fortified bread and pasta, while their nervous systems slowly degrade.
Conversely, Japan and Italy do not maintain mandatory mass folic acid fortification policies. Their public health frameworks rely on targeted, voluntary supplementation during high-risk periods (such as pregnancy) and the assumption of adequate dietary intake. While this approach effectively avoids the folic-acid-masking effect seen in the US, it places the burden of nutrient sufficiency entirely on individual dietary choices. As observed in the Italian blood donor study, without mass fortification, a massive percentage of the population fails to achieve adequate serum and red blood cell folate levels simply because they do not consume enough vegetables.
A documented clinical case from Italy perfectly illustrates the danger of the folate-B12 interaction. An Italian patient, who had been consuming high doses of folic acid, presented to an emergency department with severe balance disorders and combined degeneration of the spinal cord. Diagnostic testing revealed an extremely high serum folate level masking a profound, untreated B12 depletion. This case study underscores that excessive folic acid not only masks anemia but may actively lead to a reduction in the active fraction of Vitamin B12, exacerbating the neurological deficit.
4. Vitamin D (Calcidiol): The Global Pandemic of Hypovitaminosis and Latitude Variations
Vitamin D is fundamentally a secosteroid prohormone rather than a classical dietary vitamin. It strictly governs calcium and phosphorus homeostasis, intestinal mineral absorption, and bone metabolism. Beyond skeletal integrity, Vitamin D exerts profound pleiotropic effects, regulating immune system function, mitigating cardiovascular risk, and modulating neurodevelopment. Synthesized cutaneously upon the exposure of 7-dehydrocholesterol to ultraviolet-B (UVB) radiation, and acquired minimally through dietary sources (primarily fatty marine fish and fortified dairy), total body status is accurately measured via the serum concentration of the hepatic metabolite 25-hydroxy vitamin D.
An exhaustive systematic meta-analysis of global prevalence spanning the years 2000 to 2022, encompassing 308 studies and nearly 8 million participants across 81 countries, revealed staggering global deficits. Globally, 15.7% of individuals have serum 25(OH)D levels below 30 nmol/L (12 ng/mL), 47.9% are below 50 nmol/L (20 ng/mL), and a massive 76.6% fail to reach the optimal 75 nmol/L (30 ng/mL) threshold.
4.1 Harmonizing Clinical Guidelines: The Russian Federation and Italy
The biochemical consensus among leading European endocrinology societies including the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases (SIOMMS) and the Russian Ministry of Health is notably unified in its aggressive approach to Vitamin D sufficiency.
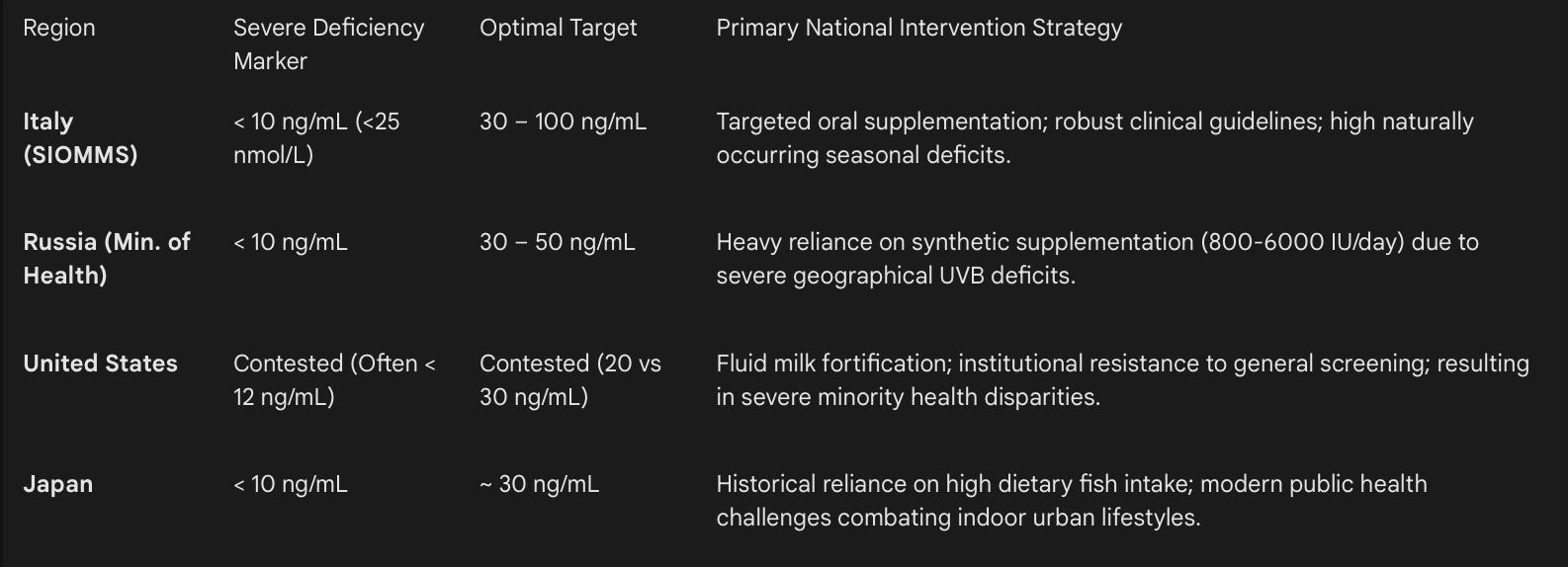
In Italy, SIOMMS categorizes 25(OH)D levels stringently to guide clinical intervention:
Severe Deficiency: < 10 ng/mL (< 25 nmol/L)
Deficiency: 10 – 20 ng/mL (25 – 50 nmol/L)
Insufficiency: 20 – 30 ng/mL (50 – 75 nmol/L)
Adequate/Optimal: 30 – 100 ng/mL (75 – 125 nmol/L)
Italian clinical guidelines recommend maintaining levels strictly above 30 ng/mL (75 nmol/L) for at-risk categories. While they discourage unfocused general population screening, they aggressively advocate oral cholecalciferol supplementation for those with established deficits, metabolic vulnerabilities, or bone-active drug prescriptions. Despite these clear clinical parameters, national surveys (such as the IV SCAI) report widespread levels of Vitamin D inadequacy in Italy. This is largely due to minimal dietary intake and reliance on natural sunlight, which is biophysically insufficient for optimal cutaneous synthesis during winter months, even at Mediterranean latitudes.
Similarly, the Russian Federation has deployed highly comprehensive clinical guidelines. Since much of Russia’s landmass resides above the 40th parallel north resulting in protracted, multi-month periods without sufficient UVB radiation, the Russian Endocrine Society and Ministry of Health advocate for widespread 25(OH)D testing in risk groups & clinical targets strictly aim for serum concentrations of 30 to 50 ng/mL (75 to 125 nmol/L).
To achieve these optimal levels in a harsh geographic climate, Russian treatment protocols recommend initial high-dose boluses (e.g., 6000 IU/day for 4 to 12 weeks) for rapid correction, followed by prolonged maintenance doses of 800 to 2000 IU/day. Clinical studies on young Russian athletes residing permanently above 55 degrees north latitude vividly confirm that aggressive cholecalciferol supplementation is absolutely mandatory to overcome geographic deficits, normalize parathyroid hormone profiles, and preserve ionized calcium levels for peak physiological performance. Close attention to this widespread deficiency is driving Russian public health policy toward progressive educational and preventative supplementation programs.
4.2 The United States: Controversial Thresholds and Systemic Disparities
The United States medical establishment remains locked in a prolonged, highly contentious scientific debate regarding appropriate Vitamin D thresholds. The US Endocrine Society’s updated 2024 guidelines notably recommended against routine screening of serum 25(OH)D concentrations in healthy adults aged 18–74, and conspicuously failed to provide a strict, unified diagnostic threshold for determining absolute vitamin D sufficiency.
This conservative stance heavily relies on randomized controlled trials (RCTs) assessing singular outcomes like bone fractures, effectively dismissing vast swaths of epidemiological and observational data that link serum levels above 30 ng/mL (75 nmol/L) to reduced all-cause mortality, lower cancer incidence, and improved autoimmune profiles. Prominent endocrinologists have sharply criticized these guidelines, pointing out that focusing solely on RCTs ignores the pleiotropic reality of Vitamin D functionality across non-skeletal tissues.
Furthermore, critics argue that the failure to establish an optimal target (such as the 30–50 ng/mL range adopted by Russia, Italy, and Poland) perpetuates severe racial health disparities. Due to the physics of cutaneous synthesis, increased melanin acts as a natural sunblock, requiring significantly more UVB exposure to synthesize equivalent amounts of cholecalciferol. Consequently, Non-Hispanic Black and Hispanic Americans exhibit exponentially higher rates of severe deficiency (levels < 30 nmol/L or 12 ng/mL).
Epidemiological census modeling indicates that roughly 6.8 million Non-Hispanic Black adults in the US exist in a state of severe, chronic deficiency. The US public health strategy of relying on fortified fluid milk is structurally flawed and highly inequitable; populations with the highest biological risk of Vitamin D deficiency also exhibit the highest genetic rates of lactose intolerance, rendering the primary national fortification vehicle virtually inaccessible to the most vulnerable demographics.
4.3 Japan: Urbanization and the Erosion of the Marine Diet
Japan presents a fascinating epidemiological paradox regarding Vitamin D. Historically, the traditional Japanese diet, exceptionally rich in fatty marine fish (a primary, highly bioavailable natural source of cholecalciferol), provided substantial prophylactic protection against hypovitaminosis D without the need for synthetic fortification.
However, contemporary longitudinal data reveals a highly concerning, shifting trend: a massive prevalence of Vitamin D insufficiency among seemingly healthy urban populations. The 2019 Japanese National Health and Nutrition Survey reported that mean Vitamin D intakes are steadily decreasing over time and have fallen significantly below the adequate intake threshold, particularly in vulnerable adolescents.
This biochemical shift is attributed to profound lifestyle changes: a drastic decrease in time spent outdoors, the heightened cultural use of UV-blocking cosmetics, and a generational, systemic drift away from traditional marine-based diets toward Westernized, highly processed food patterns. Because Japan lacks comprehensive mandatory food fortification policies for Vitamin D, relying historically on natural dietary intakes, the population remains highly sensitive to these modern behavioral shifts. Public health warnings now suggest that high-risk Japanese adolescents must aggressively reincorporate sunlight exposure and dietary modification with Vitamin D supplements to prevent the re-emergence of osteomalacia and subclinical rickets.
5. National Food Fortification Policies: A Comparative Calculus
The vast discrepancies in clinical biomarkers across these four nations cannot be fully explained by genetics, race, or latitudinal geography; they are profoundly, mechanistically influenced by national food fortification policies. The industrial fortification of foods began nearly a century ago to address acute public health crises, such as Switzerland’s iodization of salt in 1923 and the US fortification of white flour in 1943. Today, the methodology of nutrient delivery dictates the biochemical baseline of the populace.
5.1 The Economics and Efficacy of Nutrient Addition
Fortification is economically efficient but biologically blunt. The aim is to increase nutrient intake to address systemic deficiencies without causing excessive intake in sub-populations. However, the biochemistry of food processing complicates this goal. For example, adding ascorbic acid (Vitamin C) to cereal products greatly enhances the bioavailability and absorption of both native and added iron. Yet, the oxidative destruction of Vitamin C during the extreme heat of the baking process often renders this strategy cost-prohibitive, forcing manufacturers to rely on alternatives like Iron EDTA, which lack the secondary antioxidant benefits of Vitamin C.
When analyzing the intersection of macroscopic health indices and micro-fortification policies, a distinct pattern emerges. The United States utilizes heavy, mandatory fortification to mathematically patch the nutritional voids of a highly processed, obesogenic food supply. Comparative dietary data reveals that the intake of sugar, sweeteners, and beef in the US is exponentially higher than in Japan, while soy and fish intake is fractionally lower. The prevalence of clinical obesity is up to 10 times greater in the US than in Japan. Consequently, despite massive fortification programs ensuring basic daily limits are met to prevent scurvy or pellagra, the US suffers from massive rates of non-communicable, metabolic diseases, anchoring its global health index rank at an abysmal 34th place. Fortification of a toxic diet does not yield a healthy population.
5.2 Emerging Regulatory Frameworks: The Russian Approach
The Russian fortification and supplementation landscape is rapidly evolving. Recognizing the massive DALY burden of micronutrient deficiencies across a geographically isolated population, Russian authorities have fundamentally shifted their approach. Rather than relying solely on mass fortification of staple crops, Russia has recently expanded mandatory labeling and rigorous quality control for biologically active dietary supplements.
By utilizing advanced tracking codes (such as OKPD codes for fish oils and enzymes), the Russian Federation is signaling a legislative shift toward heavily regulated, direct-to-consumer supplementation to bridge dietary gaps safely. This approach acknowledges that individualized, highly regulated supplementation may be a more precise public health tool than blanket fortification, especially for fat-soluble vitamins like Vitamin D where toxicity thresholds must be managed alongside deficiency eradication.
6. Synthesis of National Architectures: Correlating Health Indices to Biochemical Standards
By synthesizing the epidemiological mortality data, specific biomarker thresholds, and macro-dietary policies, distinct national profiles emerge. These profiles mechanistically explain the trajectory from the least healthy to the most healthy populations in the developed world.
6.1 The Russian Federation: Structural Evolution in a Harsh Geography
Ranked 95th globally, Russia contends with the harshest climatic conditions of the studied nations, virtually guaranteeing widespread Vitamin D deficiency without aggressive, state-level intervention. The population historically suffers from high prevalence rates of latent iron deficiency and anemia. However, the Russian medical and scientific establishment is proactively, and aggressively, addressing these metrics. By adopting rigorous C-RIDL methodologies to establish clean reference intervals (filtering out latent pathology) and implementing aggressive Endocrine Society guidelines targeting a high 30–50 ng/mL for Vitamin D, Russia is laying the biochemical groundwork for future health. Russia’s primary barrier is not a lack of clinical stringency or awareness, but the immense socioeconomic and geographic infrastructure required to deliver adequate, high-quality nutrition and preventative screening to a vast, highly dispersed population.
6.2 The United States: High Expenditure, Low Optimization
Despite unmatched per-capita healthcare expenditure, the United States ranks 34th globally. The American epidemiological paradigm relies on mass fortification and statistical, bell-curve medicine. By accepting low B12 thresholds (often below 232 pg/mL) and fiercely debating the utility of prophylactic Vitamin D screening , the US medical system legally permits millions of its citizens to operate in a chronic state of subclinical metabolic and neurological decline.
The epidemiological data unequivocally confirms that older Americans suffer measurable cognitive consequences at B12 levels deemed perfectly “normal” by standard US laboratories. Furthermore, the over-reliance on mass folic acid fortification without corresponding B12 screening actively masks neurodegenerative pathologies. The United States demonstrates the ultimate paradox: adding synthetic vitamins to a fundamentally toxic, hyper-caloric food supply successfully prevents acute historical diseases (like rickets or neural tube defects) but fails entirely to produce a robustly healthy, metabolically stable, long-lived population.
6.3 Italy: The Vulnerability of a Venerated Diet
Ranked 2nd globally, Italy boasts exceptional longevity, low cardiovascular risk, and high overall prosperity, driven largely by the structural benefits of the Mediterranean diet and a robust, highly accessible social healthcare system. Yet, rigorous, modern national biochemical surveys expose severe, highly concerning cracks in this façade: rampant inadequacies in Vitamin D, calcium, and essential B-vitamins across multiple demographics.
Italy’s macroscopic health success is likely sustained by historical dietary momentum and a high baseline intake of polyphenols, antioxidants, and healthy fats, which mitigate oxidative stress and endothelial damage. However, as the younger population modernizes, urbanizes, and drifts from traditional, whole-food eating patterns toward processed cereals, the lack of strategic national fortification policies leaves Italians increasingly biochemically vulnerable. Advanced clinical guidelines, such as those from SIOMMS, correctly identify optimal, aggressive thresholds (e.g., >30 ng/mL for Vitamin D), but translating these high-level clinical targets into daily, population-wide sufficiency remains an unresolved public health challenge.
6.4 Japan: The Gold Standard of Preventative Biochemical Medicine
Consistently ranked in the top 5 healthiest nations globally, Japan achieves exceptional morbidity outcomes through a powerful confluence of a naturally nutrient-dense diet (characterized by high marine omega-3s, low saturated fat, and high phytochemical intake) and extremely stringent, preventative clinical standards.
By recognizing serum B12 levels below 500 pg/mL as functionally, neurologically deficient , Japanese medicine aggressively treats the biochemical precursors of neurodegeneration decades before they manifest as overt dementia or structural brain damage. While Japan faces emerging, serious challenges with Vitamin D insufficiency due to rapid urbanization and the abandonment of traditional fish-heavy diets by younger generations , its foundational approach to laboratory biomarkers serves as the gold standard in nutritional epidemiology. Japanese healthcare demands biomarker levels that actively support optimal biological function, rather than settling for the statistical averages of a declining population.
7. Strategic Implications for Global Nutritional Epidemiology
The exhaustive comparative analysis of vitamin deficiency norms across the United States, Russia, Japan, and Italy yields profound, actionable insights into the mechanics of macroscopic public health and longevity.
First, clinical reference intervals are highly susceptible to shifting, deteriorating population baselines. When a laboratory defines “normal” by taking the mathematical average of an increasingly unhealthy, aging, or metabolically compromised population, the medical system inadvertently normalizes and institutionalizes chronic disease. The Russian adoption of LAVE methodologies to filter out latent pathology before establishing a baseline is a critical, necessary evolution in laboratory science that other nations must adopt.
Second, the epidemiological data firmly establishes that the healthiest nations (Japan and Italy) achieve maximum longevity primarily through the consumption of complex, whole-food dietary matrices, rather than the mass fortification of ultra-processed foods. However, Japan’s drastically superior management of neurological health is inextricably linked to its demand for higher, proactive biochemical thresholds, specifically regarding Vitamin B12. Treating patients to achieve optimal physiological states (e.g., >500 pg/mL for B12 and >30 ng/mL for Vitamin D) rather than simply keeping them out of acute crisis is the hallmark of advanced preventative medicine.
Finally, the reliance on mandatory mass fortification in nations like the United States must be urgently coupled with updated, aggressive clinical diagnostic thresholds. Fortifying the food supply with high-dose synthetic folic acid while simultaneously ignoring subclinical B12 depletion creates a highly dangerous epidemiological environment where macrocytic anemia is masked, while irreversible spinal and cognitive neurological damage advances undetected.
To elevate global health indices, national health ministries must transition away from population-derived statistical reference ranges and universally adopt outcome-based clinical decision limits. Only by strictly defining biochemical normalcy through the exacting lens of optimal cellular, neurological, and metabolic function can modern medical systems pivot from merely managing chronic decline to genuinely fostering human healthspan and longevity.